

What is changing for Medicare Part B services in the skilled nursing facility setting effective January 1st, 2017?
On Wednesday, November 2, 2016, the Centers for Medicare & Medicaid Services (CMS) issued a final rule that updates payment policies and payment rates for services furnished under the Medicare Physician Fee Schedule (PFS) on or after January 1, 2017.
The final changes are summarized below. Refer to our previous article for the background about the upcoming changes.
What Will Change on January 1st?
1- Therapy Cap:
The Therapy cap for 2017 will increase from $1960 to $1980 for 2017.
Therapy Cap History: There is one therapy cap for outpatient occupational therapy (OT) services and another separate therapy cap for physical therapy (PT) and speech-language pathology (SLP) services combined. The therapy caps apply to outpatient therapy services [Part B] furnished in all settings. The therapy cap amounts are updated each year based on the Medicare Economic Index (MEI). Specifically, the annual caps are calculated by updating the previous year’s cap by the MEI for the upcoming calendar year and rounding to the nearest $10.00. Increasing the CY 2016 therapy cap of $1,960 by the CY 2017 MEI of 1.2 percent and rounding to the nearest $10.00 results in a CY 2017 therapy cap amount of $1,980.
2- Therapy Exceptions Process:
The Therapy Exceptions Process will continue for 2017 with use of the KX Modifier on the billing claim to indicate services above the cap are reasonable and necessary and that there is documentation of medical necessity for the extended services. By using the KX modifier, the therapist is attesting that the services above the therapy caps are reasonable and necessary and that there is documentation of medical necessity for the services in the beneficiary’s medical record.
{Do you know when your residents are over the cap? Did you know that the billing person applying the KX code is doing so on your behalf, indicating that you attest to the necessity of these services?}
Therapy Exceptions Process History: An exceptions process for the therapy caps has been in effect since January 1, 2006. Originally required by section 5107 of the Deficit Reduction Act of 2005 (DRA), which amended section 1833(g)(5) of the Act, the exceptions process for the therapy caps has been extended multiple times through subsequent legislation as described in the CY 2015 PFS final rule with comment period (79 FR 67730) and most recently extended by the MACRA. Authority to provide an exceptions process for therapy caps expires on December 31, 2017. CMS tracks each beneficiary’s incurred expenses annually and counts them towards the therapy caps by applying the PFS rate for each service less any applicable multiple procedure payment reduction (MPPR) amount. After expenses incurred for the beneficiary’s outpatient therapy services for the year have exceeded one or both of the therapy caps, therapy suppliers and providers use the KX modifier on claims for subsequent services to request an exception to the therapy caps. By using the KX modifier, the therapist is attesting that the services above the therapy caps are reasonable and necessary and that there is documentation of medical necessity for the services in the beneficiary’s medical record. Claims for outpatient therapy services over the caps without the KX modifier are denied.
3- Manual Medical Review Process:
The Manual Medical Review Process will continue for 2017 for claims over the $3700 threshold. However, not all claims exceeding the therapy threshold will be reviewed. In 2017, targeted reviews will occur for therapy providers with a high claims denial rate and/or those with aberrant billing practices as compared to peers.
{Do you know when your resident hits the $3700 mark in a calendar year? Do you know if your billing department is getting denials? Do you think your billing practices (# of units billed per session, days per week, etc. ) match your peers? Or are you an outlier?}
Manual Medical Review Process History: Since October 1, 2012, under section 1833(g)(5)(C) of the Act as amended by the Middle Class Tax Relief and Jobs Creation Act of 2012 (MCTRJCA) (Pub.L. 112–96), CMS has been required to apply a manual medical review process to therapy claims when a beneficiary’s incurred expenses for outpatient therapy services exceed a threshold amount of $3,700. Just as there are two separate therapy caps, there are two separate thresholds of $3,700, one for OT services and one for PT and SLP services combined; and incurred expenses are counted towards these thresholds in the same manner as the caps. Under section 1833(g)(5) of the Act, as amended by section 202(b) of the MACRA, not all claims exceeding the therapy thresholds are subject to a manual medical review process as they were before. Instead, since MACRA, CMS will do a more targeted medical review on these claims using factors specified in section 1833(g)(5)(E)(ii) of the Act as amended by section 202(b) of the MACRA, including targeting those therapy providers with a high claims denial rate for therapy services or with aberrant billing practices compared to their peers. The manual medical review process required under section 1833(g)(5)(C) of the Act expires at the same time as the exceptions process for therapy caps, on December 31, 2017.
4- New Therapy Evaluation Codes:
The {old} evaluation codes will be deleted. Say goodbye to:
- 97001: PT Evaluation
- 97003: OT Evaluation
The codes will be replaced with a set of tiered codes based on level of complexity. The complexity of the evaluation will be coded based on low, moderate or high levels. Say hello to:
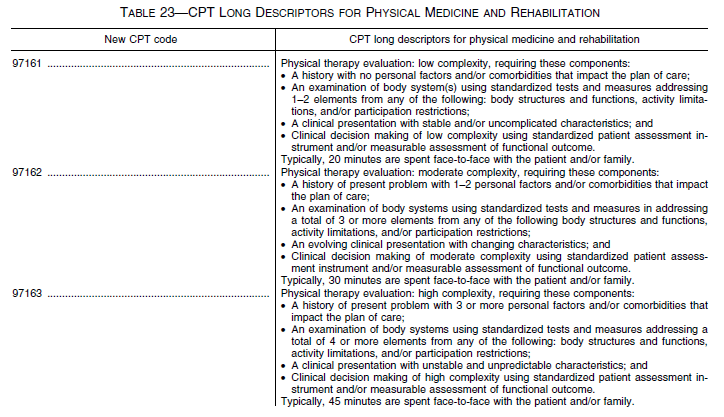
- 97161: PT Evaluation – Low complexity- 20 face-to-face minutes
- 97162: PT Evaluation – Moderate complexity- 30 face-to-face minutes
- 97163: PT Evaluation – High complexity- 45 face-to-face minutes
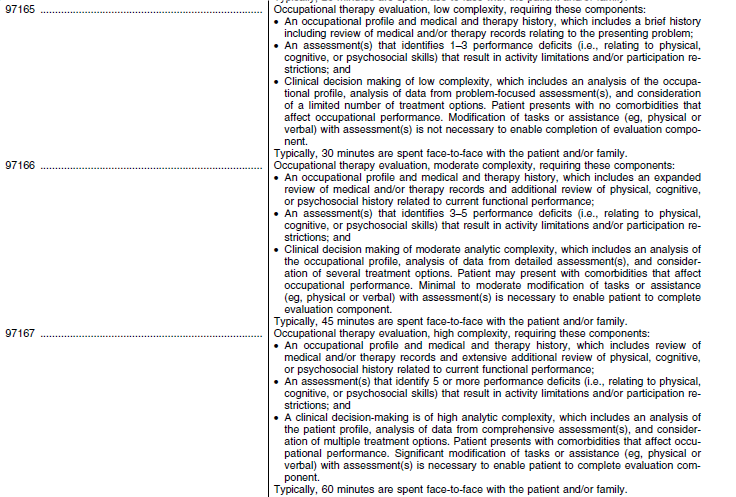
- 97165: OT Evaluation – Low complexity- 30 face-to-face minutes
- 97166: OT Evaluation – Moderate complexity- 45 face-to-face minutes
- 97167: OT Evaluation – High complexity- 60 face-to-face minutes
Here are the descriptors for each code. Please note the codes now include face-to-face time.
5- New Therapy Re-Evaluation Codes:
The {old} re-evaluation codes will be deleted. Say goodbye to:
- 97002: PT Re-evaluation
- 97004: OT Re-evaluation
The codes will be replaced with the following:
- 97164: PT Re-evaluation- 20 face-to-face minutes
- 97168: OT Re-evaluation- 30 face-to-face minutes
Here are the descriptors, including face-to-face time requirements, for the re-evaluation codes:


A Note About Face-To-Face Time Requirements
The face-to-face time requirements for the same complexity category are different for PT and OT. For example, a moderate complexity PT evaluation has a face-to-face time of 30 minutes, which matches the face-to-face time requirements for a low complexity OT evaluation. The re-evaluation codes also have different times allocated; PT at 20 and OT at 30 minutes. Why the difference?
CMS has clarified in the Final Rule that these ‘‘typical times’’ for face-to-face interaction for PT and OT Evaluation/Re-evaluation codes are included as a frame of reference and do not represent a minimum coding requirement. Just as the typical times included for each E/M code represent the physician face-to-face time with the patient, the typical times in the new PT and OT CPT codes represent the typical face-to-face time of the physical or occupational therapist with the patient.
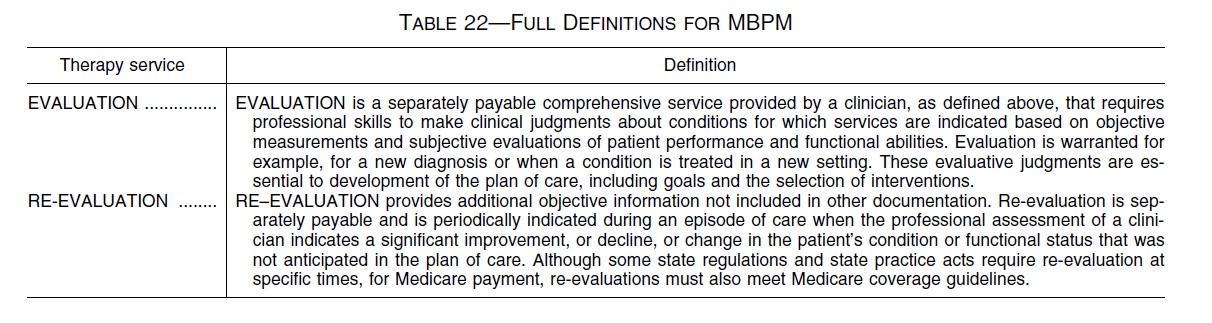
Evaluation and Re-Evaluation Definitions Revised
CMS is reminding physical and occupational therapists in the Final Rule about instructions in Chapter 15 of the Medicare Benefit Policy Manual regarding the reporting of a both the evaluation and re-evaluation codes (MBPM, Chapter 15, section 220). Of note, to be separately payable, the re-evaluation requires a significant change in the patient’s condition or functional status that was not anticipated in the plan of care. The MBPM full definitions follow in Table 22 and will be updated in Chapter 15 of the Medicare Benefits Policy Manual.
 In Summary
In Summary
 In Summary
In SummaryWe have a month left to familiarize ourselves with the new codes and definitions so that we will be ready to code accurately and responsibly in January. Keep in mind that even if all code complexities will “pay the same” in 2017, this will not be the case moving forward. CMS has indicated that they will analyze how therapists use the codes and levels in 2017 and then make determinations on their value based on the data they collect. The patterns that we establish now will impact us later! So….Code Choices matter!
Now is the time to review your documentation process. Are you documenting about co-morbidities? Are you documenting on all of the “performance deficits” found on evaluation? How many minutes are you currently documenting for your evaluation?Are you using standardized tests? {Don’t forget, the Therapist Toolbox has tests specific to the geriatric population that you can print out and use.}
Keep yourself in the loop and ahead of the curve! Look for our upcoming New CPT Evaluation Code educational materials.
In Your Corner,
Dolores
Dolores Montero, PT, DPT, RAC-CT, RAC-CTA
Montero Therapy & MDS Resource Team
www.MonteroTherapyServices.com
Visit our Just Ask Q&A Forum – Get your questions answered!