
What’s staying, What’s Going, what’s new, & how to manage it all
You may have heard….the MDS world is changing on October 1st, though October changes in the Skilled Nursing Facility (SNF) setting are nothing new. Change occurs every year, without fail. However, this October 1st, the changes are on a much larger scale.
Minimum Data Set (MDS) Items, language, and entire methods of calculating scores and measures that have existed for decades will change. That’s big.
The focus here will be on MDS Section GG and the associated changes. Let’s look at what’s staying, what’s leaving, what’s new, and how to handle it all!
Section GG
Until now, Section GG has only been required for Medicare Part A residents at the start and end of Medicare. Yes, your therapy EMR may have had the Self Care and Mobility items weaved into your therapy evaluations, re-certifications and discharges, however, that data never made it to a MDS that was submitted to CMS unless the resident was traditional Part A at the time.
On October 1st and beyond, those familiar GG Self Care and Mobility items will not only be required for Medicare Part A residents, they will be required for all residents regardless of payor, for all non-Medicare (PPS) MDS assessments.… Admission….Quarterly…Annual…Significant Change…and on top of that, there are new items for Self Care and Mobility.
More on that in a minute.
First, we can’t look at Section GG without first mentioning Section G.
Why? The reason Section GG is making its way on to every MDS and continues to grow is solely due to the fact that Section G will retire on September 30th, along with its rule of 3, extensive and limited assist language, and fancy algorithm. If you are not familiar with Section G, to say it has played a major role in SNF life is an understatement.
Section G is weaved into the very fabric of the SNF, beyond the MDS. Section G has been the backbone for all long-term care residents on every federally required MDS, since the late 80’s. Until now, Section GG has only applied to Medicare Part A residents. Big difference!
Section G’s current responsibilities:
So yes, G has been a big deal, and now Section GG has some big shoes to fill come October 1st!
The Matching Game
If Section G is going away on October 1st, and Section GG is growing, there must be some correlation between the two, right?
The Final MDS 3.0 Item Sets have been released, Section G is gone, and we know for sure what the “new” GG looks like. But CMS has not yet released all the “behind the scene connections” that GG will have to all G’s old roles…..Care Area Triggers, Quality Measures…. This info will be released in the next 1-2 months per CMS, as will the Final RAI Manual.
Let’s look at Section G items and see what happened to each item in relation to Section GG. If you are a visual learner, these pictures are worth 1,000 words.
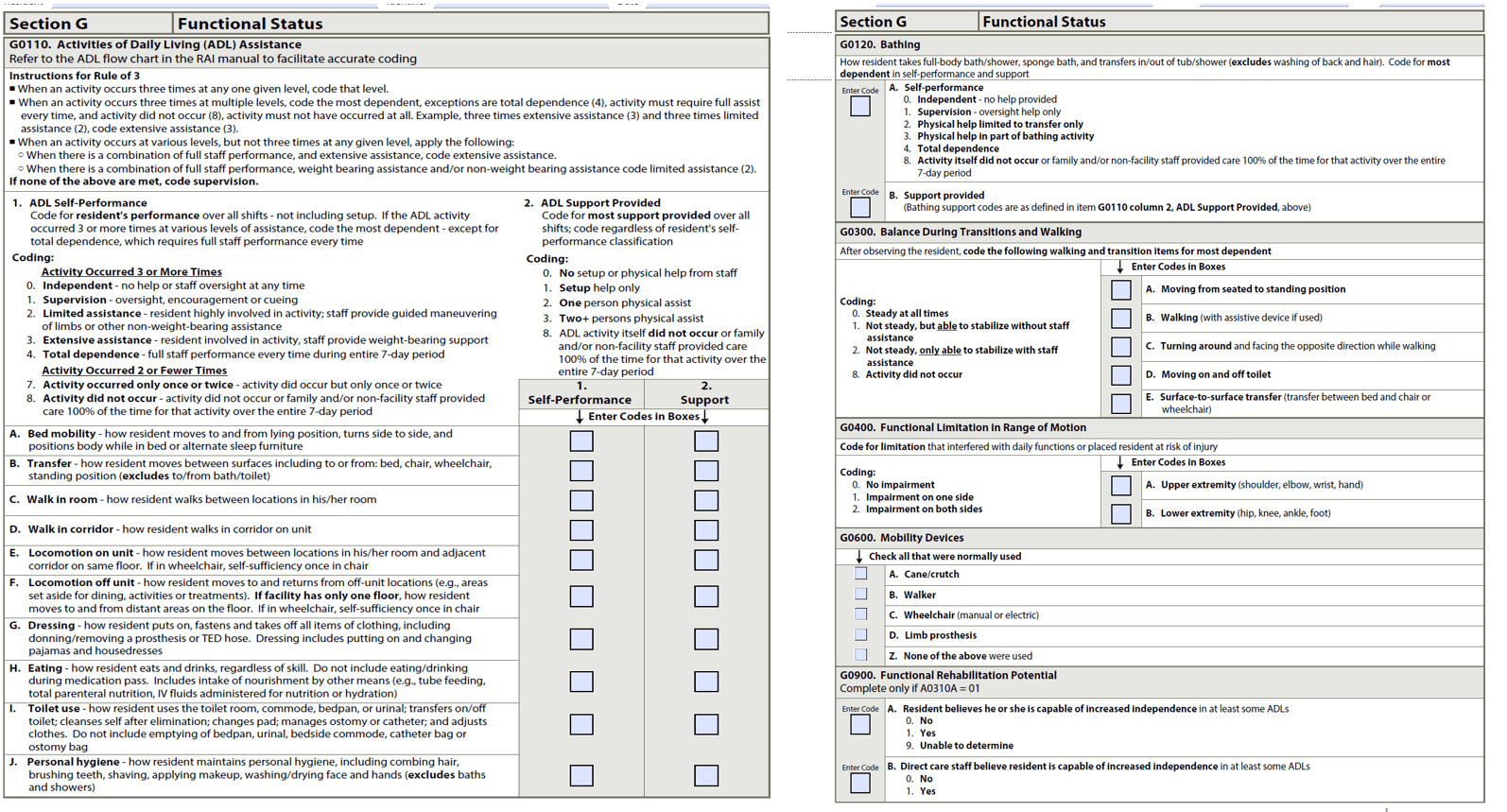
This is the current Section G. The left half contains the ADL items (G0110) and the right has Bathing (G0120), Balance (G030), Range of Motion (G0400), Mobility Devices (G0600), and Rehab Potential (G0900).
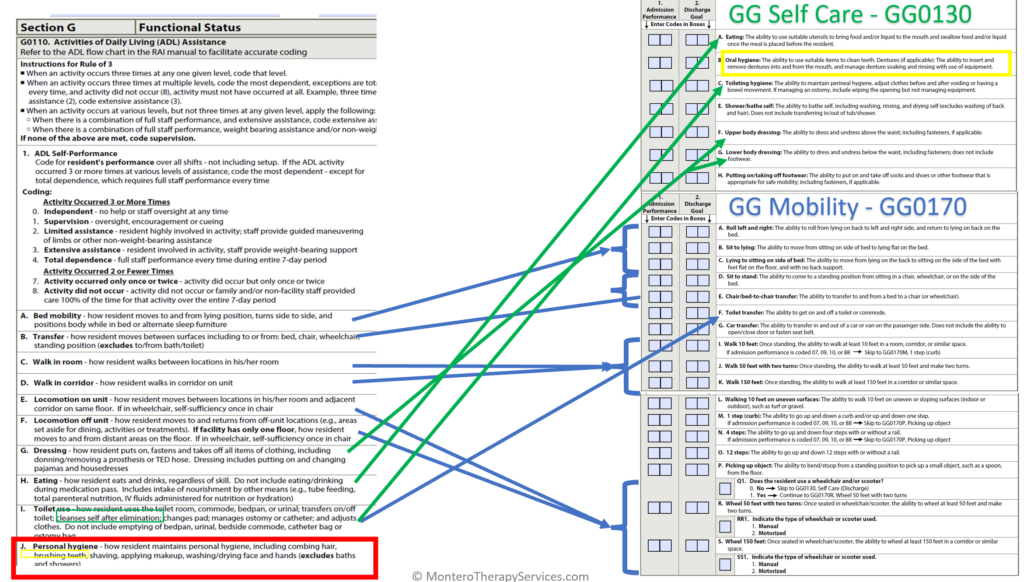
Now let’s look at which items from G are currently represented on Section GG.
New GG Self Care Item: Personal Hygiene
When looking at the ADL section of G side–by-side with the current Section GG below, you can see that each ADL item A-J already has a similar item in Section GG Self Care or Mobility.
Except one. Personal Hygiene (J).
Section G’s Personal Hygiene includes brushing teeth, as well as combing hair, shaving, washing hands, and more. Section GG has Oral Hygiene, but this item does not cover all the hygiene tasks listed in Personal Hygiene.
A new Section GG Self Care item GG0130(I) “Personal Hygiene” will be added to the Admission, Annual, Quarterly, Significant Change & Discharge MDS assessments for all payors. These are the “OBRA,” or Federally required by the Omnibus Budget Reconciliation Act of 1987 (OBRA ’87) MDS assessments.
The new Section GG Self Care items that go into effect 10/1/23 are shown here, including the new Personal Hygiene question and definition:
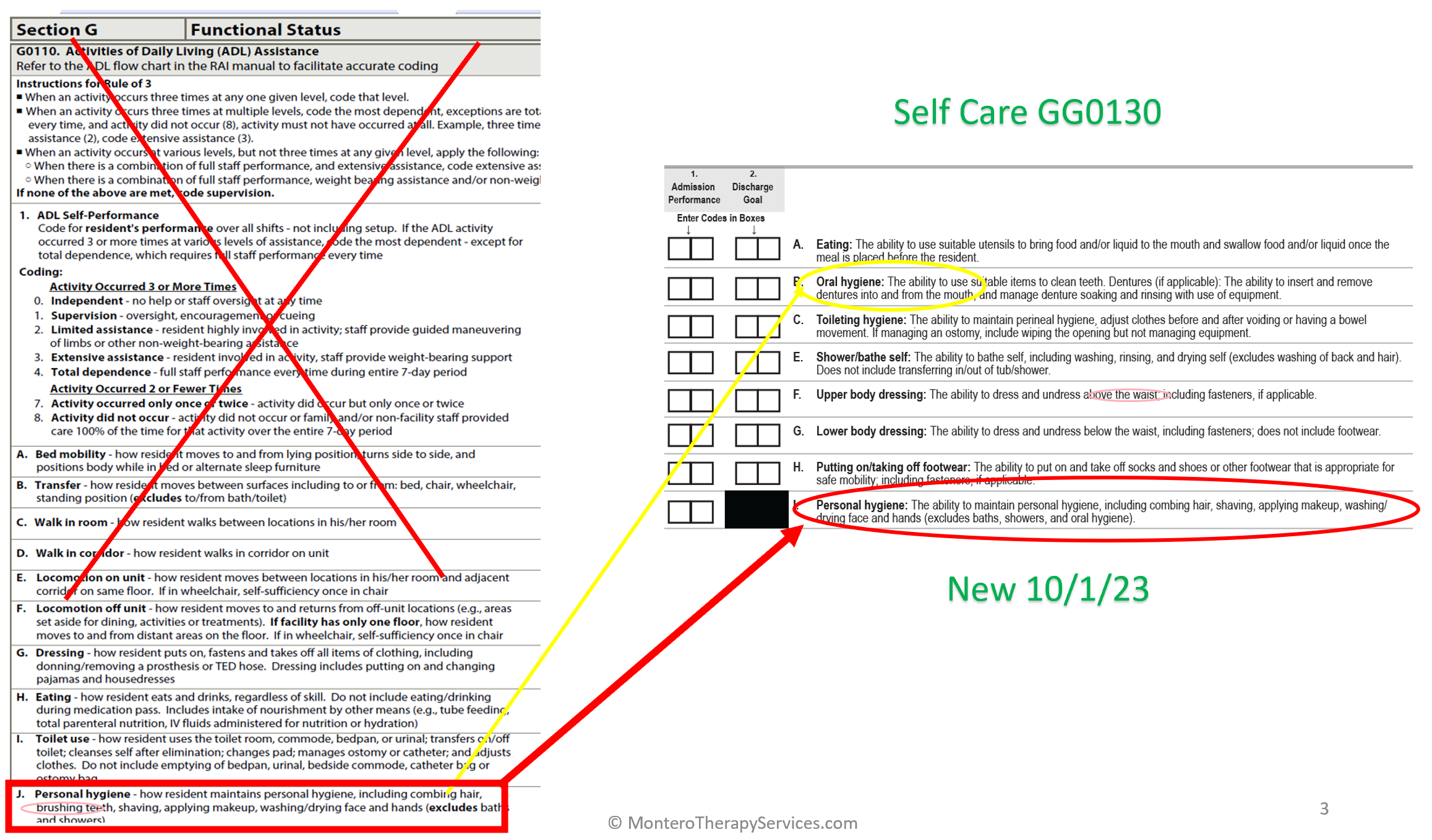
With this addition, all the Functional Status ADL items from Section G0110 now have a matching counterpart in Section GG. The descriptions of each item may not be exact, but the general items and concepts match.
New GG Mobility Item: Tub/Shower Transfer
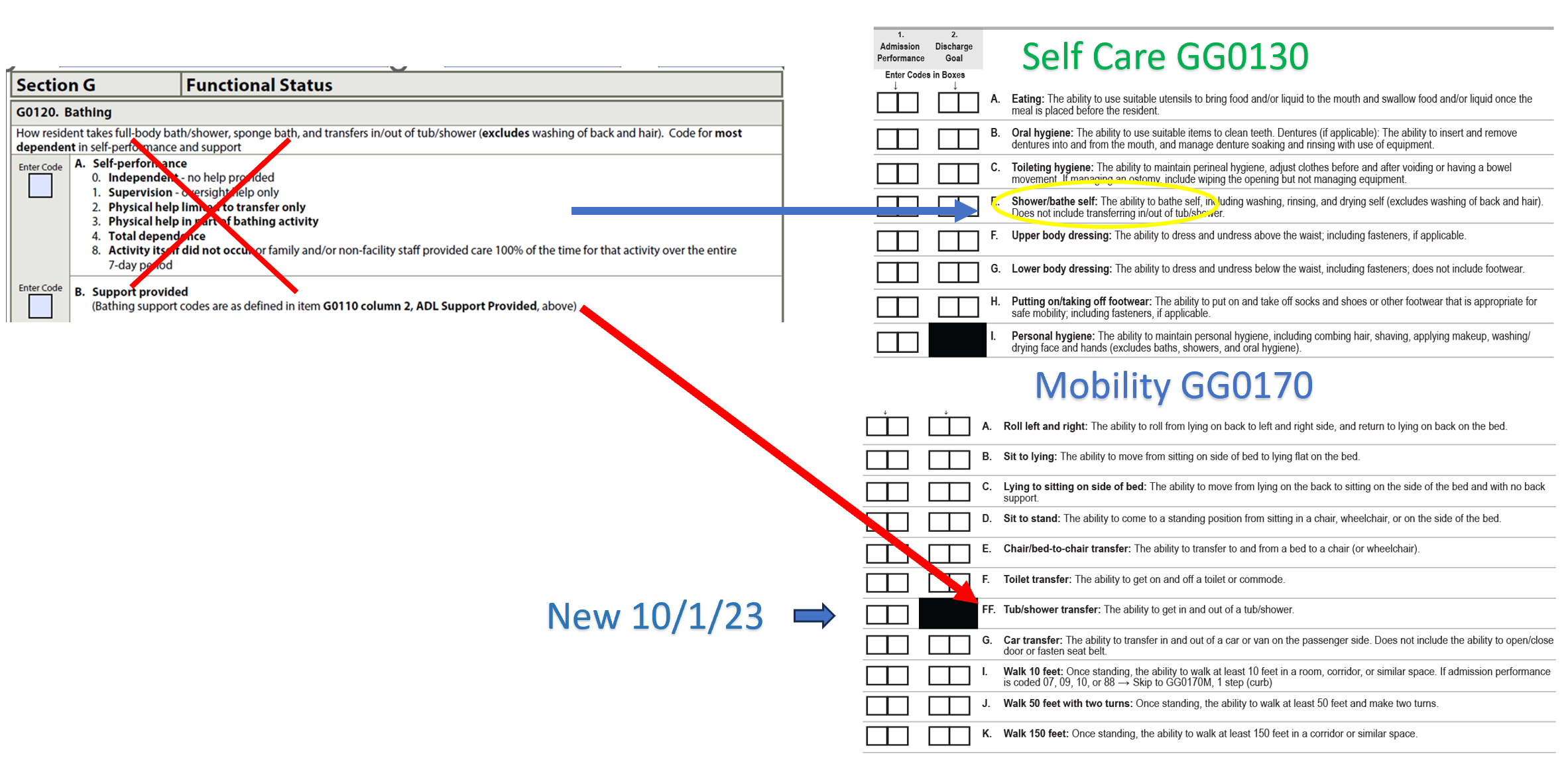
In Section G, Bathing (G0120), was always a separate item, split from the other items in the ADL section. Section G Bathing includes coding the resident’s ability to bathe, as well as the transfer to the tub/shower. We know that the current Section GG already had “Shower/Bathe Self” as a Self Care item, but this only told half the story, as GG did not have an item to represent the transfer portion of the task.
As shown below in the new GG, “Shower/Bathe Self” under Self Care will remain, and “Tub/Shower Transfer” is added to the Mobility set. This item will be added to the OBRA assessments: Admission, Annual, Quarterly, Significant Change & Discharge MDS assessments for all payors effective 10/1/23.
It is important to note here that because Shower/Bathe Self is under the Self Care Section, and Tub/Shower Transfer is under the Mobility Section, and some therapy EMRs allocate the Self Care items to Occupational Therapy assessments and Mobility items to Physical Therapy assessments, there will need to be discussion as to how your therapy team [and your therapy EMR] will assess these items. Personal Hygiene is clearly part of an OT assessment, though tub/shower transfers could potentially be addressed by either PT or OT. Ensure your EMR is flexible to allow cross-assessment between disciplines.
Remaining Section G Items
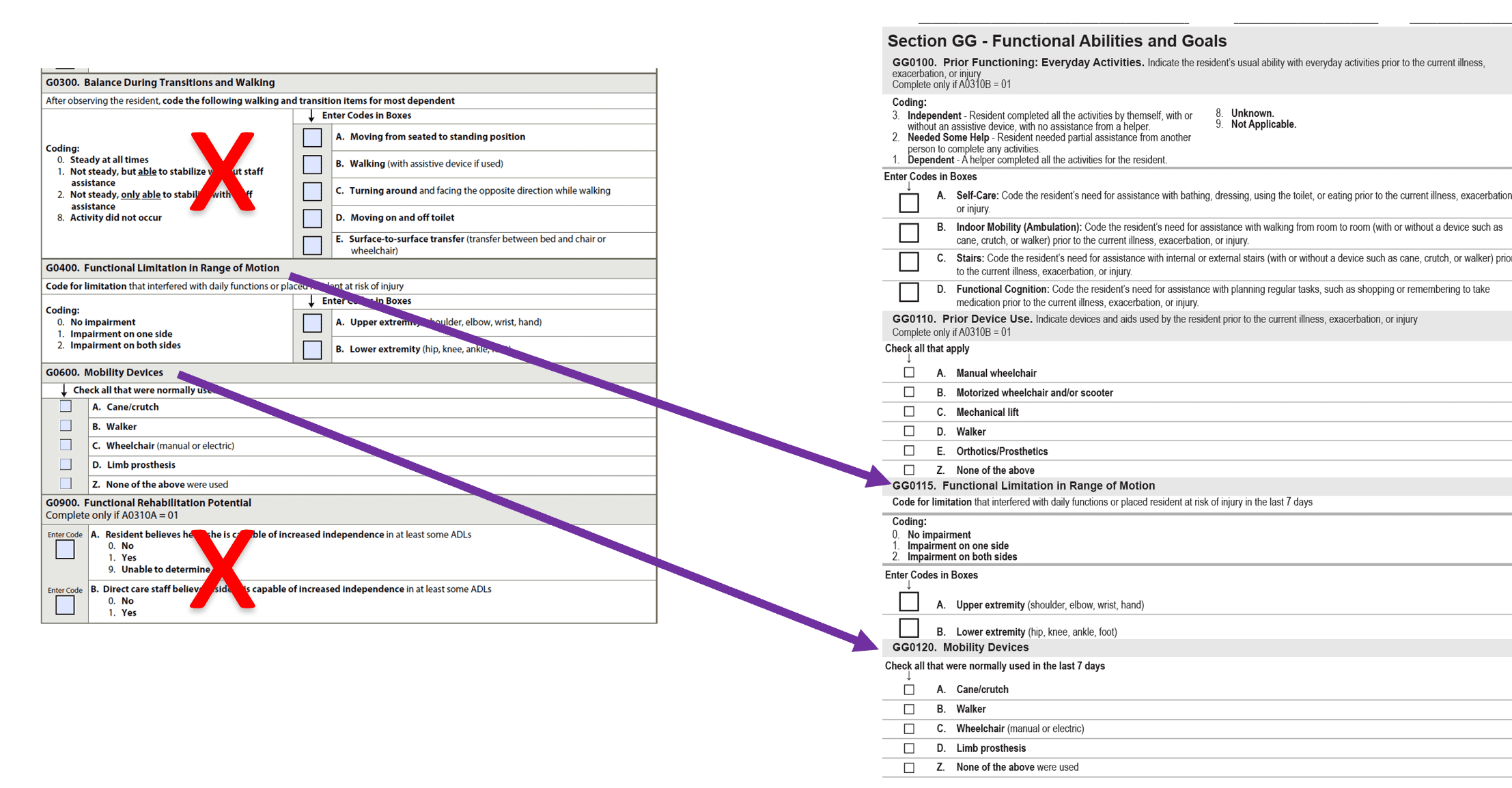
Of the remainder of Section G items, only half make it to Section GG. Functional Limitation in Range of Motion and Mobility Devices are transferred “as is” to Section GG0115 and GG0120 respectively. These will now be required on the OBRA assessments, and will continue to be required on the Medicare PPS 5 Day. The Balance and Functional Rehab Potential sections did not make the cut, though don’t worry, the flavor of these items are incorporated elsewhere on the MDS.
This illustrates what is transferring from G to GG, and what is eliminated:
What & When
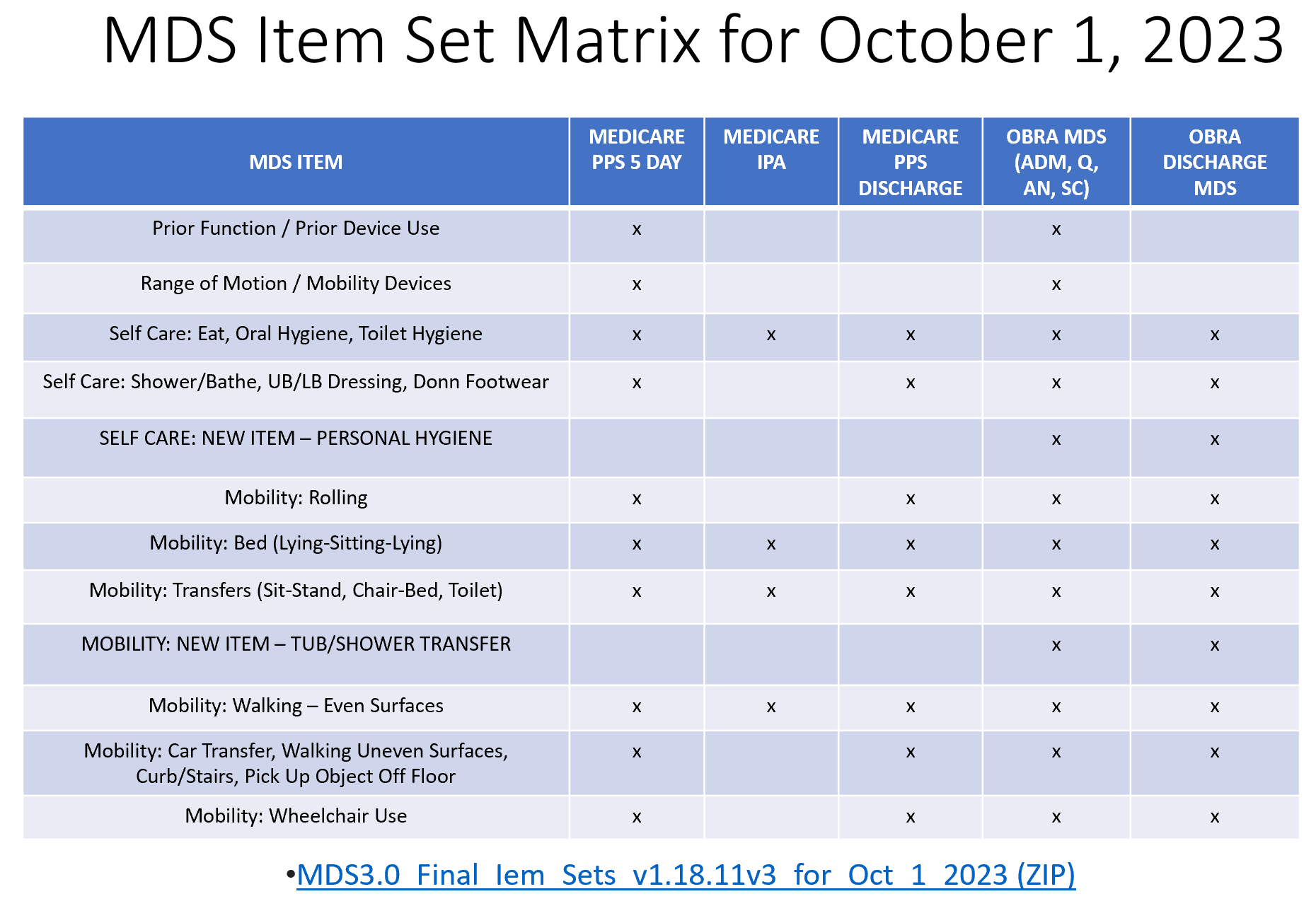
The new GG Self Care item, Personal Hygiene, and new GG Mobility Item, Tub/Shower Transfer, won’t be collected for Medicare Part A assessments, unless they are combined with an OBRA assessment. Functional Limitation in Range of Motion and Mobility Devices will be collected on the Medicare 5 Day and all OBRA assessments.
The MDS Item Set Matrix below shows the GG items and corresponding MDS assessments.
Juggling the ARD and Data Collection
Managing the Assessment Reference Dates (ARD), “lookback” or documentation collection window for each type of assessment, Medicare and non-Medicare, will be key moving forward. There are unique requirements for each type of assessment, and missing the opportunity to document in the required window may mean not capturing resources that will be needed for Quality Measures (QM), 5 Star, SNF Quality Reporting Program (QRP) and Patient Driven Payment Model (PDPM) reimbursement.
What are the Section GG data collection periods now that GG is on all the MDS assessments?
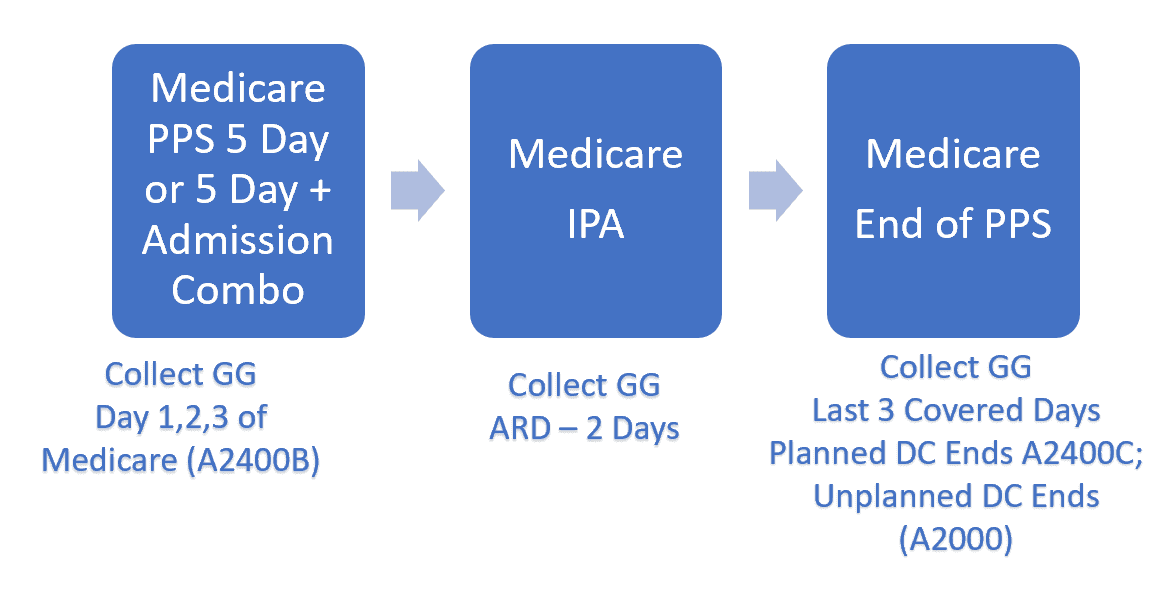
Breakdown for Medicare Part A Residents:
Breakdown for Non-Medicare Residents:
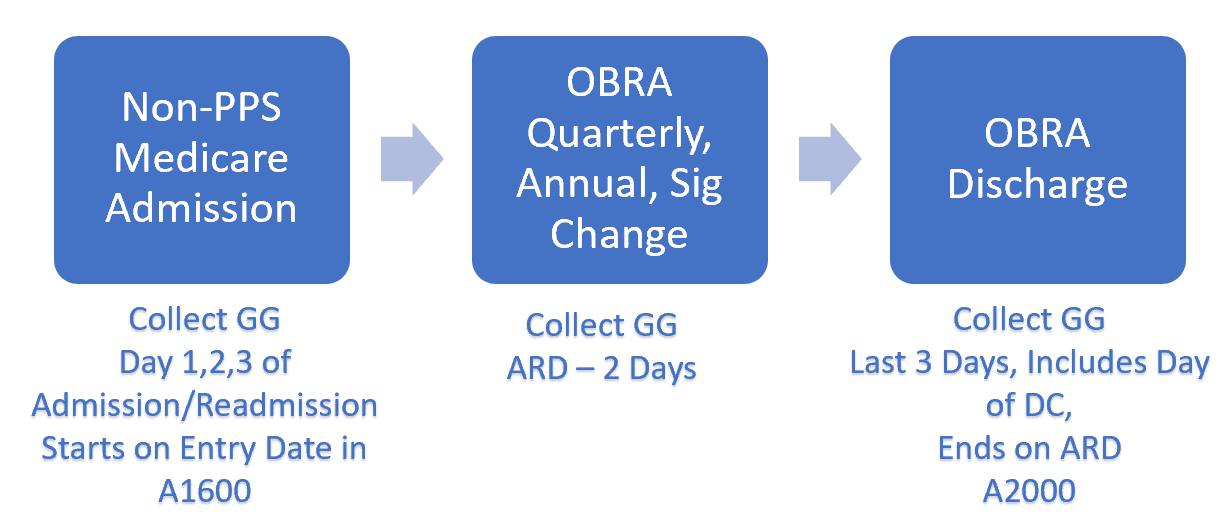
Keep in mind that for stand-alone OBRA Admissions, the GG 3-day collection window is independent of the ARD, and both require their own unique data collection. GG data collection windows will take some getting used to.
Bye-Bye Algorithm
One of the biggest changes with the transition from Section G to Section GG for all MDS assessments is the loss of the algorithm to determine how to code functional status.
Once upon a time, MDS nurses had to view all ADL documentation in the lookback and manually code Section G [onto a paper MDS] using the “rule of 3.” Once EMRs came on the scene, Section G ADLs could be determined by letting the EMR use the rule of 3 algorithm to analyze all data entries, typically made every shift by direct caregivers, and determine coding with the click of a mouse.
Section GG determination does not use an algorithm. Coding is based on IDT input and the clinical assessment of a qualified professional to review data from a small 3-day window of time and determine “usual performance.” Usual, meaning not the best, not the worst, not what happened the most, not what happened the least, and definitely not the average. Try making an algorithm for that!
Coding Section GG for all the non-Medicare Part A MDSs is now the same scenario for the Medicare residents. One, there needs to be data to review for the GG items in the window, and two, the MDS nurse (or other qualified professional) needs to use clinical judgement to assess & code each item.
a few things to think about
This was just a snippet of what is changing on the MDS October 1st. Stay tuned for a review of additional MDS Section changes, as well as a deeper dive into Section GG. The Final RAI Manual is due out very soon, and once this, as well as the Quality Measure information is released, all the pieces can be put together.
For now, digest the G to GG changes included here, and how they will impact your current role and contribution to the MDS process.
It is clear that CMS’ intent is to have the GG items replace the G items on the MDS and beyond. Consider the following during your conversations:
- Who will document?
- How will you transition documentation from G to GG in your facility?
- Will nurse assistants begin documenting for all GG items every shift? This may not be necessary, but ensure at least the Self Care Items and a bulk of the Mobility Items are documented on daily. The State Operations Manal requires that SNFs have a system in place to ensure residents “attain and maintain” highest level of function or risk F-675 Tag for Quality of Life.
- Limiting the Mobility GG items for nursing assistants to document on daily may be a good idea. For example, car transfers, stairs and picking up objects off the floor may be overkill. Possibly include documentation on all items monthly, quarterly or just in the ARD lookback.
- When and how will nurse assistant training for Section GG be completed?
- Section GG for Medicare Part A payment:
- The new GG Self Care and Mobility items do not impact the Function Score or PDPM payment.
- Consider keeping GG documentation for Medicare Part A residents [and any other payor that uses PDPM methodology] for the nursing and therapy staff only, especially until the nurse assistant documentation can be audited to ensure they are using the new coding key correctly with daily documentation.
- Medicaid State Case Mix:
- If you are a Medicaid case mix state still using RUGs, you will have no choice but to keep Section G daily documentation (and make sure your EMR keeps it as well or you will be manually coding using the rule of three), as you will still have Section G on the Optional State Assessment (OSA).
- Documentation will only be needed for the 4 Late Loss ADLs, and only needs to be collected in the 7-day ARD lookback. See if your EMR has the option to add this feature. Or consider another method of data collection (ie: nurse manager interview caregiver and document status each shift during lookback only).
- Does therapy currently participate in state case mix MDS quarterly screens? Keep in mind the ARD and lookback window for inclusion of GG information for any evaluations completed.
The upcoming MDS changes present an opportunity for therapy’s role to evolve with contributing to the MDS for all residents regardless of payor source. More interdisciplinary team (IDT) input into resident functional abilities will ultimately contribute to the best plan of care, with the goal of attaining and maintaining highest level of function for each resident, and therapy is the perfect discipline to evaluate self care and mobility!
For now, here’s wishing Section G a happy retirement!
Additional resources for your exploration:
Any questions, Just Ask!
In Your Corner,
Dolores
Dolores Montero, PT, DPT, RAC-CT, RAC-CTA
Montero Therapy & MDS Resource Team
MonteroTherapyServices.com