
CMS released the Medicare Part A Skilled Nursing Facility Prospective Payment System Final Rule, {AKA SNF PPS Final Rule}, and just as expected, therapy professionals will have a chance to catch their breath! The rule changes for 10/1/20 are minimal in comparison to years past, resulting in a document to digest that is less than half the typical size. The 40 page Final Rule can be accessed from the Federal Register webpage HERE
Let’s look at the highlights that are most pertinent to SNF therapy professionals.
Medicare Part A Payment Rate Changes
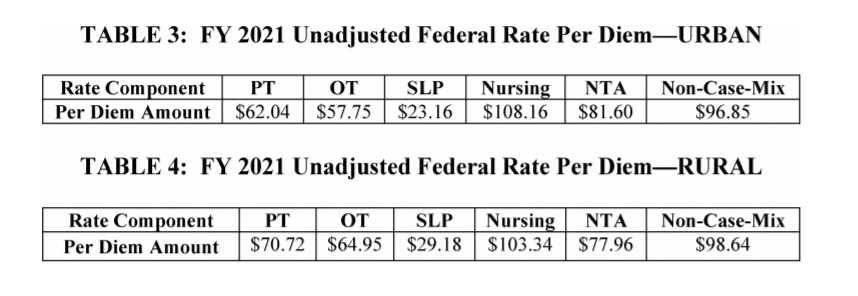
The Federal Per Diem rates are updated annually. The payment update for FY2021 is an increase of 2.2% from last year, which equates to approximately $750 million more for SNFs. These are the unadjusted rates that when multiplied by the case mix index values then determine each PDPM Case Mix Group rate. The Urban rates are just as they were in the Proposed Rule and the Rural rates changed slightly in both the SLP and Non-Case Mix Components.
Medicare Part A PDPM Changes – Case Mix Index Values
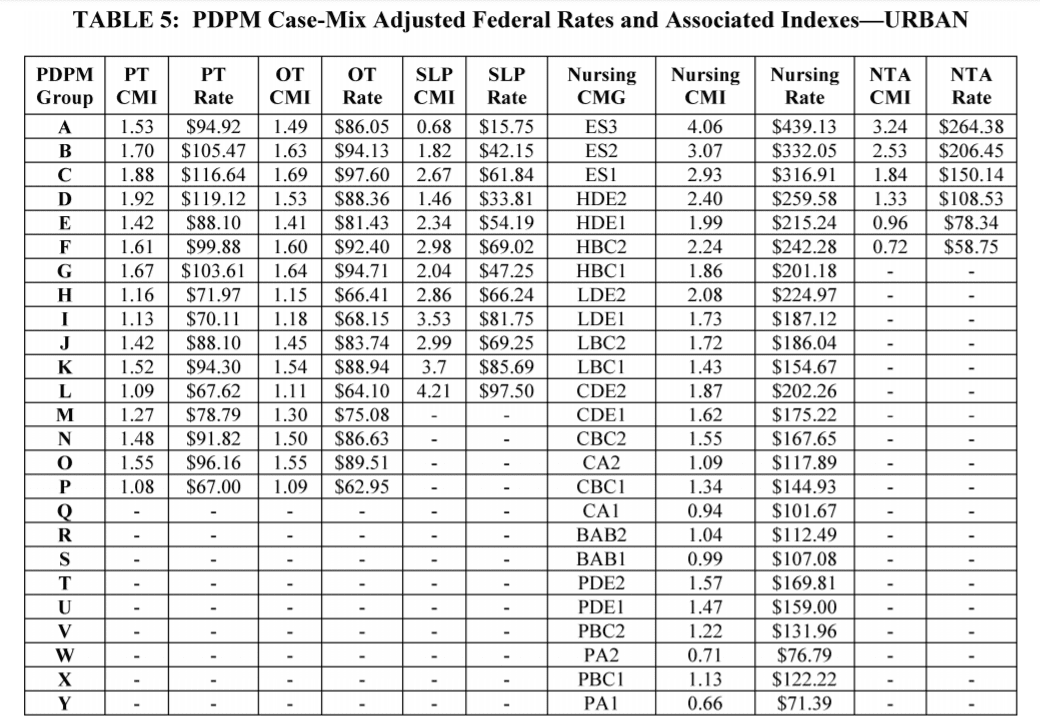
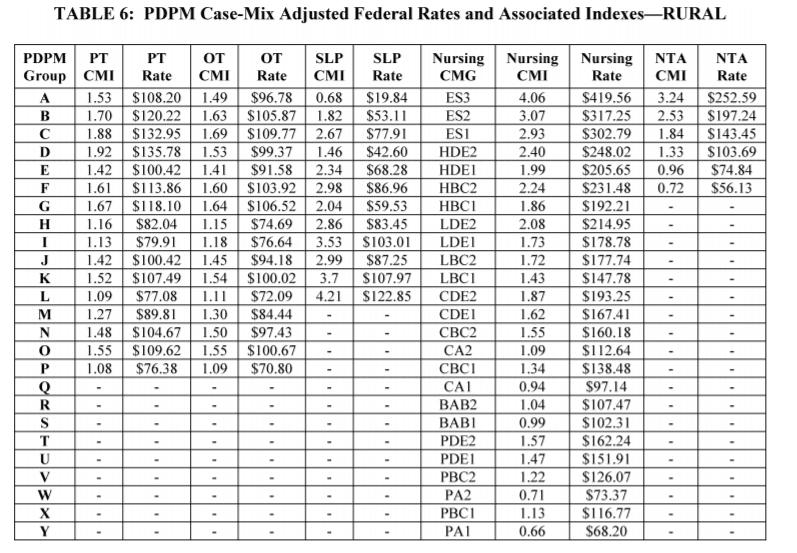
Case Mix Index values for each of the PDPM Components, PT, OT, Speech, Nursing and Non-Therapy Ancillary, did not change from FY2020 for Urban SNFs and only slightly changed in the SLP Group for Rural SNFs for FY2021. When multiplied by the Unadjusted Federal Per Diem Rate shown above, Case Mix Group rates will look like this for 2021 for Urban and Rural facilities.
Changes In Wage Index – Geographical Locations – For Medicare Part A Calculation
Providers are deemed “urban” or “rural” for purposes of calculating the labor portion of the daily rate, a factor in determining the overall daily rate for a facility. Using wage index values specific to location to adjust the labor portion of the rate is done to reflect the wage differences throughout the country. [Reimbursement rates are different depending on where you live.] The Final Rule makes changes to a small number of counties… some previously listed as urban will switch to rural and vice versa. The result of these changes? 42% of SNFs will experience a decrease and 54%, an increase in the wage index values.
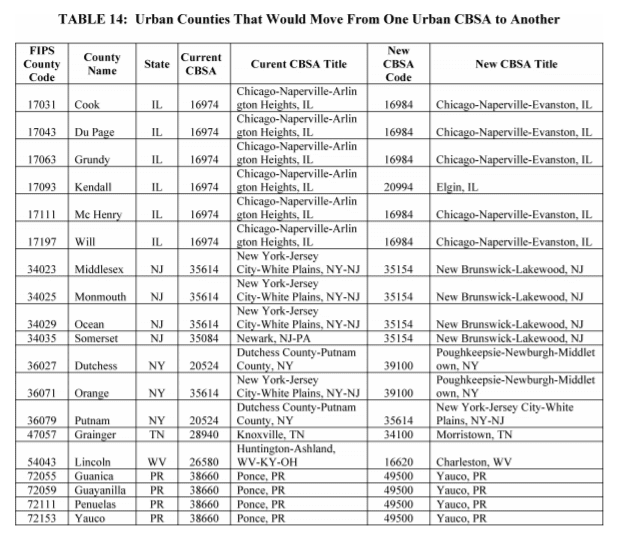
Use the list below to see if your county was impacted.
Counties Changing from Urban to Rural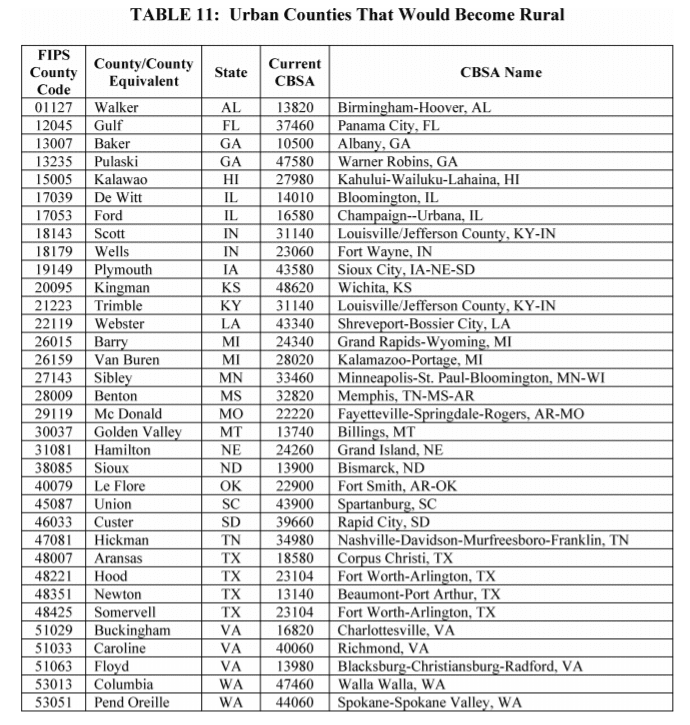
Counties Newly Classified as Urban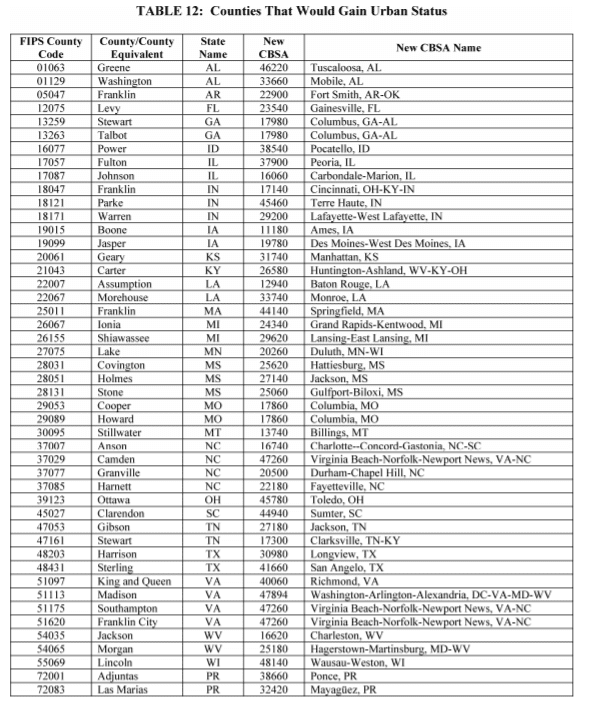
Urban with a Name or Code Change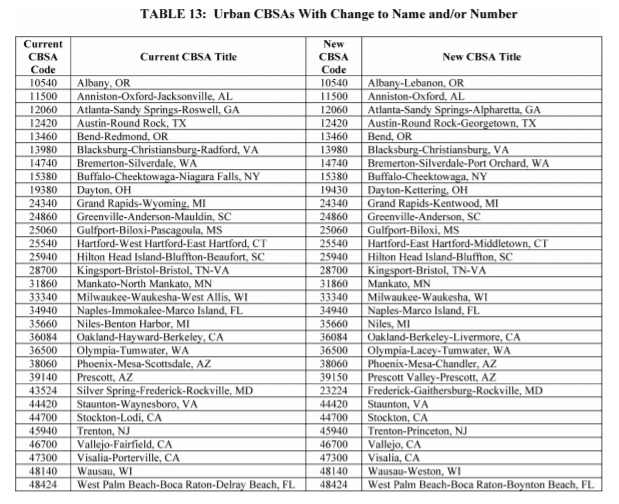
Urban Counties Switching to New Code / Grouping
Not sure if you are urban or rural?
Use the Wage Index Table below to look up your county. You need to know your facility classification to calculate the exact reimbursement rates for each Case Mix Group and Part A daily per diem rate.
- CMS Wage Index Home Page
- CMS-1737-F Wage Index Tables for FY 2021 – Final (ZIP)
- Use our Urban or Rural Look Up Tool for FY2021
Medicare Part A PDPM Changes – ICD-10 Code Mapping for PT and OT Component
ICD-10 Codes used in MDS Section I0020B as the primary reason for SNF Part A covered care are used for case mix classification under PDPM. Using the Mapping Tool provided by CMS, each ICD-10 Code can be mapped to 1 of 4 PT and OT Clinical Categories as shown here, or identified as a Return to Provider code [meaning this code cannot be used in Section I0020B of the MDS]. In the Final Rule, CMS has made some adjustments to the mapping, as well as added and deleted additional codes.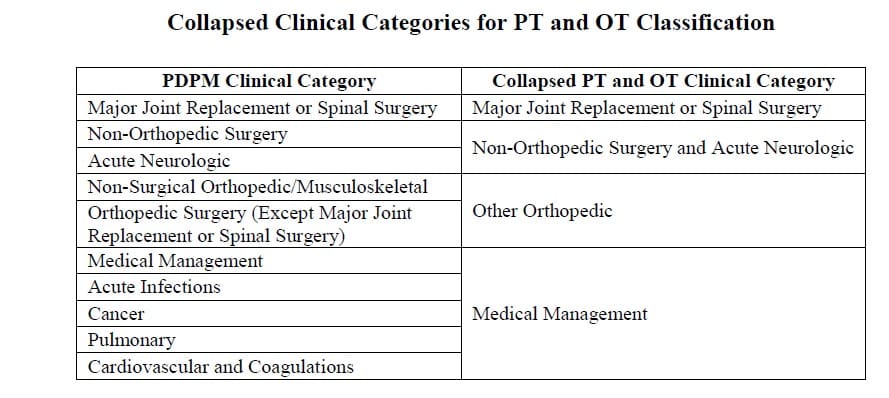 First, as a result of the National Emergency, ICD-10 Code U07.1 “COVID-19” was added to the current list of codes (this code is in effect now) and maps to Pulmonary and Medical Management. To view the CMS ICD-10 Mapping Tool updated 3/31/20 with the new code, CLICK HERE. By 10/1/20, a new mapping tool will be released for use to include the additional code changes, as follows:
First, as a result of the National Emergency, ICD-10 Code U07.1 “COVID-19” was added to the current list of codes (this code is in effect now) and maps to Pulmonary and Medical Management. To view the CMS ICD-10 Mapping Tool updated 3/31/20 with the new code, CLICK HERE. By 10/1/20, a new mapping tool will be released for use to include the additional code changes, as follows:
- Remapping certain Cancer ICD-10 Codes to allow for combination with specific Section J surgical procedures to increase the category from Medical Management to either “May Be Eligible for the Non-Orthopedic Surgical” category, or “May be Eligible for One of the Two Orthopedic Surgery Categories.” (Codes range from C15 to C80.1 and D37.09 to D49.7).
- Adjusting the default clinical category mapping for codes linked to “Ortho Surgery” or “Major Joint” to prevent automatic mapping when no surgery occurred. Includes S32.031D Lumbar Fracture, S32.19XD Sacral Fracture, S82.001D to S82.002J Patella Fractures. These will now map to “Non-Surgical Orthopedic” and if coded in Section J as surgery, then will potentially bump to the “May be Eligible for One of the Two Ortho Surgery Categories.”
- Remapping a handful of ICD-10 Codes for Spinal Stenosis (M48-M48.08) from “Non-Surgical” to be eligible for “One of the Two Orthopedic Surgical” categories if specific items in Section J are checked.
- Remapping a handful of ICD-10 Codes for Surgical Aftercare to be eligible for “Non-Orthopedic Surgical” categories if specific items in Section J are checked.
- Aftercare following transplant: Heart Z48.21; Kidney Z48.22; Liver Z48.23; Lung Z48.24; Heart-Lung Z48.280; Multi-Organ Z48.288; Other Z48.298
- Aftercare following surgery for: Nervous System Z48.811; Circulatory System Z48.812; Respiratory System Z48.813; Digestive System Z48.815; Genitourinary System Z48.816;
- Assigning “Return to Provider” for some of the less specific fracture codes all related to the patella (ie: S82.009A, S82.013A, S82.016A, S82.023A, S82.026A, S82.033A, S82.036A and S82.099A)
Medicare Part A PDPM Changes – ICD-10 Code Mapping for the Non-Therapy Ancillary Component
Non-Therapy Ancillary Component points are derived from either checking specific diagnoses on the MDS, or adding the ICD-10 Code to Section I8000. Codes for use in I8000 with corresponding point value are provided by CMS in the NTA Mapping Tool. In the Final Rule, there is 1 noted change in the list of ICD-10 codes used to identify “Complications of Specified Implanted Device or Graft.” The ICD-10 codes that can be included in I8000 of the MDS to capture 1 NTA point for this category will be reflected in the new mapping tool to include the seventh digit “D,” indicating “subsequent encounter” vs those that currently end in “A,” indicating initial encounter. The codes affected will be T82.310A-T85.89XA.
Changes to the Minimum Data Set (MDS)
In December of 2019, CMS posted a draft of the MDS 3.0 item set to be implemented 10/1/20. Major changes were proposed, including the removal of Section G from OBRA assessments. Then on March 19th, 2020, CMS announced that the MDS changes planned for October 1, 2020 would be delayed. Read HERE for more information.
However, we are not getting away with “no changes” for October 1st. In May, CMS posted updated MDS 3.0 Item Sets (Version 1.17.2) and related technical specifications. These changes allow the PDPM HIPPS Code calculation on OBRA Assessments (Admission, Quarterly, Annual) when they are not combined with a 5 Day PPS MDS. Remember, Section GG is needed to calculate a PDPM Function Score. Therefore, Section GG was added to the OBRA Assessments for October.
Section GG has a different set of instructions for the OBRA Assessments. If the OBRA MDS is completed for State PDPM purposes (ie: if your state is using PDPM scores to calculate state Medicaid payments), then Section GG will be completed. However, since there is no “PPS Day 1,2 and 3” to use for the GG data collection, the MDS instructions state that the ARD and 2 days prior to the ARD will make up the 3 day period of data collection needed to determine “usual performance.” Also, if GG is completed for state purposes only, the Discharge Goal Column does not need to be completed, only the Performance Column. Here is what the directions for Section GG now look like:

This change will allow State Medicaid Agencies to collect and compare RUG-III/IV payment codes to PDPM ones and thereby inform their future payment models. Facilities will need to confirm with State Medicaid Agencies if your State will be requiring the calculation of the PDPM payment codes on the OBRA assessments when not combined with a 5-day SNF PPS assessment.
Nothing is changing for Medicare Part A completion of Section GG….this is only if an OBRA MDS is done and a PDPM score is needed for state purposes.
Changes to CMS Medicare Part A Quality Programs
While a 2.2% increase in the Medicare Part A rates for FY2021 sounds wonderful, the full impact of facility reimbursement also depends on 2 of the CMS Quality Measure Programs. As we know, the SNF VBP program automatically deducts 2% from each facility (so your 2.2% increase is now 0.2%). The SNF then has the opportunity to earn a portion of that 2% back for “good behavior.” The SNF QRP program can also deduct another 2% from Part A reimbursement, though this only happens if your SNF is submitting PPS MDSs with incomplete data.
- SNF Quality Reporting Program (SNF QRP)
- The SNF QRP is the program behind Section GG, as well as other MDS data collection to measure multiple areas of care. Think skin….falls….function. There are no proposed changes to the SNF QRP for FY2021! Data collection for the multiple measures in this program will continue, and facilities will continue to be subject to a 2% Part A payment penalty for submission of Part A MDS’s with missing (dashed) data in select items.
- SNF Value-Based Purchasing Program (SNF VBP)
- The SNF VBP Program is the one that reduces Medicare Part A payments to all SNFs by 2% and then allows for an opportunity to recoup all or part of the 2% by demonstrating success with the established Quality Measure. There is currently only 1 Measure with this program and the only change for FY2021 is the formal name of the measure. The original name “SNF 30-Day All Cause Readmission Measure” will now be “Skilled Nursing Facility Potentially Preventable Re-admissions after Hospital Discharge.” In essence, this measures if the resident was readmitted back to the hospital within 30 days of being discharged from the hospital. The Rule includes the Achievement Threshold and Benchmark data for FY2023 as pictured here. There were no other changes to this program for FY2021.

In Summary
This October 1st, SNF therapy professionals will only see a few changes, as compared to last October 1st when our world flipped upside down. While we may have a chance to catch our breath from rule changes, there is no rest for the weary! We can take these Medicare changes in stride and continue to work through a global pandemic while fighting for the quality of care our residents deserve.
In the next few months, we may continue to see additional regulatory changes due to the National Emergency and COVID-19, and as October 1st approaches, we may see the expiration of some of the Waivers in place. SNF professionals have a lot to keep track of these days! Visit our SNF COVID-19 Resource Page to help stay on top of the changes.
As always, if you have any questions, send them to our Just Ask Q&A Forum and we will reach out to you to get your questions answered.
In your corner,
Dolores Montero, PT, DPT, RAC-CT, RAC-CTA
SNF Rehab & MDS Compliance Team | www.MonteroTherapyServices.com