

Every October 1st the Skilled Nursing Facility (SNF) setting can expect changes. What are the changes proposed by CMS this year?
We’ve broken down the SNF Prospective Payment System (PPS) Proposed Rule and pulled out what SNF therapy and MDS professionals need to know. The information in this document is organized as a resource and teaching tool for staff. The information is divided into the 3 main topics of the Rule tied to Medicare Part A and incorporates the pending changes for each:
- Part A Rates, PDPM and the MDS
- SNF Quality Reporting Program (SNF QRP)
- SNF Value Based Purchasing (SNF VBP)
A solid foundation in each of these areas will allow you to help your facility succeed. Take it 1 piece at a time….
Medicare Part A Rates, PDPM Changes & MDS Changes
Medicare Part A Rates
The Federal Per Diem rates are updated annually, and for Part A, we typically see an increase, unlike the Part B yearly therapy reductions. On 10/1/26, the rates for Part A have a proposed net increase of 2.4%, which equates to an overall increase in payment to SNFs in FY2027 of $888 million distributed between the 15,000+ SNFs today.
To put the proposed 2.4% increase in perspective, if all 15,000+ SNFs received equal “raises” this would equate to less than $60,000 more this year, as compared to the 3.2% increase last year, or $77,000 more per SNF. Not a great raise in either case, but at least moving in the right direction!
This is how the new rate is determined:
- [(Market Basket increase of 3.2% + Forecast Error Correction of 0%) – 0.8% Productivity Adjustment (MFP)] = 2.4%.
Below are the proposed Unadjusted Federal Per Diem rates used to calculate each Patient Driven Payment Model (PDPM) Case Mix Group (CMG) rate.


Now that we have daily per diem rate information, let’s put this together with changes to the Case Mix Index values in the next section to outline the individual rate for each Case Mix Group.
Medicare Part A PDPM Changes – Case Mix Index Values
Case Mix Index (CMI) values for each of the PDPM Components, PT, OT, Speech, Nursing and Non-Therapy Ancillary, are assessed annually and updated as needed. These values are important as they assign “weight” to each of the CMGs, and when multiplied by the daily per diem rates in the prior section, determine the rate for each individual CMG.
The CMI values for each of the 5 components for 10/1/26 will remain the same as last year. The dollar values will be different, of course, due to the rate changes, but the CMI values will remain the same. (This makes updating our calculators much easier!) CMI values for each CMG can be found in the chart below.
The proposed “adjusted” daily rates for each of the case mix groups are derived by multiplying the Unadjusted Federal Per Diem Rate with the CMI value assigned to each CMG. These are the pieces needed in order to calculate the total daily rate.
Total Daily Rate = PT + OT + SLP + Nursing + NTA + Non-Case Mix Rate
As a reminder, all of the CMG scores are derived based on how the MDS “trigger questions” are answered. The Non-Case Mix Group Rate is a “flat rate,” not tied to the MDS.
For example, using the Urban chart below, a HIPPS Code of KACD1 represents TK [PT $111.53] + TK [OT $105.25] + SA [SLP $18.51] + ES1 [Nursing $373.92] + ND [NTA$128.33] + Non-Case Mix Rate [$120.89]. The total base rate for this HIPPS Code would be $858.43 per day.
Proposed FY2027 (Urban) *Visit our PDPM Resource page for more info

FY 2027 PDPM case-mix adjusted federal rates and associated indexes (ZIP)
The total rate per day fluctuates based on what “PPS day” it is. Days 1-3 see a higher rate due to the NTA Component paying triple, and days 21-100 see a rate reduction as the PT and OT Components slowly decrease in value throughout the stay. The base rate reflects payment for days 4-20, when there are no variables that impact the rate involved.
Changes In Wage Index – Geographical Locations – For part a rate calculation
In the section above, we demonstrated how to calculate the daily per diem rate. To take this rate and transform it into the rate that your SNF will receive, requires another piece of the puzzle…. the Wage Index (WI).
CMS categorizes SNFs as Urban or Rural and assigns a unique WI value to each county or state. This WI is a variable used to take the Total Daily Per Diem Rate and adjust it up or down based on where you live.
The total daily rate explained in the section above is comprised of a Labor Portion and a Non-Labor Portion. The WI is used to adjust the Labor Portion to get your location-specific rate.
Total Daily Rate = Labor Portion + Non-Labor Portion
Your SNFs Total Daily Rate = (Labor Portion x Your SNFs Wage Index) + Non-Labor Portion
CMS updates these WI values each year. The proposed Wage Index Tables for FY 2027 can be found here:
The Wage Index for your SNF can change from year to year. Since the WI is a variable in the calculation of your daily rate, a decrease in your WI will mask the full benefit of the Part A rate increase. For FY2027, a large number of locations had a decrease in the WI, and will impact the SNFs in those regions. Use this tool to see what your proposed WI is for FY2027.
In each Rule, CMS includes a daily rate calculation example for a mock SNF. This can be found in Table 8, 9 and 10 of the Proposed Rule. This is worth a look to help you bring the information together.
Make note of whether your SNF is Urban or Rural, and your area WI. Not sure if your SNF is classified as urban or rural? Use the Wage Index Look Up Tool HERE and plug that into the PDPM Calculator to get your rates.
Medicare Part A PDPM Changes: ICD-10 Code Mapping For PT, OT + Speech Components
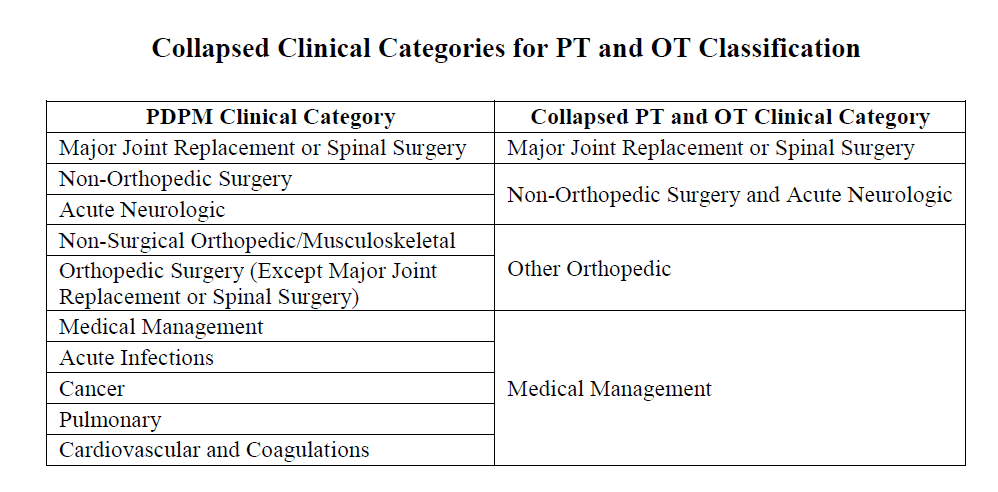
The ICD-10 Code selected for MDS Section I0020B as the primary reason for SNF Part A covered care is used for case mix classification under PDPM….. and a lot hinges on this diagnosis. Using the Mapping Tool provided by CMS, each ICD-10 Code can be mapped to 1 of 4 PT and OT Clinical Categories as shown here, or identified as a Return to Provider (RTP) code.
In other words, Return to Provider Codes can’t be used to represent the primary reason for skilled care in Section I0020B. The code that is used in this Section will fall into 1 of the 4 collapsed Clinical Categories below, thus, determining the PT/OT Component grouping.
It is important to note, Section I0020B is the only place where RTP codes can’t be used. RTP simply means “the diagnosis is not valid to represent the primary reason for a Part A stay.” These RTP codes can be placed in Section I8000 of the MDS or on the billing claim if they accurately represent an active diagnosis for the resident.
Each year, CMS makes modifications to the mapping of certain ICD-10 Codes. This year, CMS is not proposing any changes in this area.
Below is the ICD-10 Mapping File for all PDPM ICD-10 Mapping. The mapping files are needed to determine the Case Mix Group for the PT/OT, Speech and NTA Components. Your EMR may have some of this information built in, however, using the source documents from CMS is your best bet.
PDPM ICD-10 code mapping (ZIP) – Proposed FY2027
Changes to the Non-Therapy Ancillary (NTA) Component
Potential changes to the NTA Component were highlighted in prior years and information was collected regarding these potential changes in a prior RFI.
Things have been pretty quiet for the past 2 years, and no changes are expected in this area for FY2027. If you are interested in the potential NTA changes CMS discussed, we explained them in detail in our review last year.
mDS Changes Coming 10/1/26
There are no proposed MDS changes for 10/1/26! Really!
The Rule, does however, address major potential changes down the road (FY2031) which would not only add a few more “assessment types,” but would also require completion and submission of assessments for non-traditional Medicare Part A residents receiving skilled care. In other words, residents in a skilled stay paid by Medicare Advantage or Private Plans would require PPS Assessments to be completed and submitted.
The draft item sets needed to support this future change can be found at this link, and outline the options in the following 3 MDS sections. The Language includes “Other Skilled Care Assessments.”
- Section A0310 Type of Assessment
- Section A1405 Payer Information – Primary Payer
- Section A2405 Other Skilled Care Stay
FY27_Proposed_Rule_SNF_All_Payer_draft_mockups_MDS__508.pdf (PDF)
More information can be found in the SNF Quality Report Program section below, as the proposed MDS changes are a direct result of the expansion of the Quality Measure Program.
before we move on to Quality Measures…
Though there are no major changes to PDPM in the Proposed Rule, the Rule did discuss a major future change we all need to be aware of…..
A Request for Information (RFI) is included in the Rule for a change to the PDPM payment system to address Case Mix Upcoding, or “Case-Mix Creep,” as CMS called it.
The RFI focuses on ways CMS could address what they are deeming “observed Case Mix upcoding,” or improper coding for higher scores and payment. The “ways” to combat the creep include targeted reductions in specific PDPM components, or reductions across the board.
We have much more to say about the Case Mix Creep.
Moving forward….
Changes To CMS Medicare Part A Quality Measure Programs
If you are not already heavily involved in your SNF Quality Measure Program processes, NOW is the time. As these Measure Programs grow and grow, don’t get left behind. By understanding the Measures and Programs, SNF therapy and MDS professionals can be a godsend to their facility. Here, we break down each program and what will be changing.
- SNF Quality Reporting Program – SNF QRP
- SNF Value Based Purchasing Program – SNF VBP
SNF QRP
The SNF QRP is the program that started small over 10 years ago [remember when Section GG was new?] and has now ballooned into the program with the most measures. This is a pay for reporting program, meaning, SNFs are required to report measure data on specific MDS items, and if not reported, facilities can be subject to a 2% Part A payment penalty.
CMS wants your data. The penalty occurs when information is missing, not for poor outcomes. [yet]
Here is a link to all the MDS questions that, if not filled out, will trigger the payment penalty if the threshold is met. This list is in effect for CY2026… data collected in CY2026 impacts payment in FY2028.
The list of item sets (MDS questions) continues to grow, making the attainment of submitting 100% of the required quality measure data collected on at least 90% of all PPS Part A assessments to avoid the penalty is a challenge!
Make sure MDS staff have the list of MDS items above. These are the MDS items being collected NOW that will potentially impact FY2028 Annual Payment Update (APU) Determination.
The SNF QRP works in 2 time tables. The collection of data NOW [reporting period] will impact your payment in the FUTURE.
In addition to submitting 90% of all Part A MDS assessments with no missing data, SNFs also need to submit 100% of data for the COVID-19 and Influenza Vaccination for Healthcare Personnel to the CDC National Healthcare Safety Network (NHSN). If info is missing on the MDS or vaccination info is not sent timely to the CDC, the 2% payment penalty will apply. This does not leave much room for error… and this is about to get even more challenging…. read on.
SNF QRP Changes for FY2027
There are no “new Measures” for the SNF QRP in the Proposed Rule.
There are 2 Measures for proposed removal, both related to COVID-19 vaccinations, due to “no longer aligning with current clinical guidelines or practice.” The removal would be for FY2028.
- MDS-based Measure “COVID-19 Vaccine: % of Residents Who Are Up to Date“
- Beginning with residents discharged on or after October 1, 2026, SNFs would no longer be required to collect and submit the Patient/Resident COVID–19 Vaccine measure data to CMS.
- CMS is proposing to remove this question/data element (O0350) from the MDS effective October 1, 2027. Until then, it can be dashed without a penalty.
- The National Healthcare Safety Network reporting Measure, “COVID-19 Vaccination Measure Among Healthcare Personnel”
- Proposed for removal from the SNF QRP in FY2028, meaning that SNFs that do not report CY 2026 HCP COVID–19 Vaccine measure data would not be penalized for the FY 2028 annual payment update under the SNF QRP.
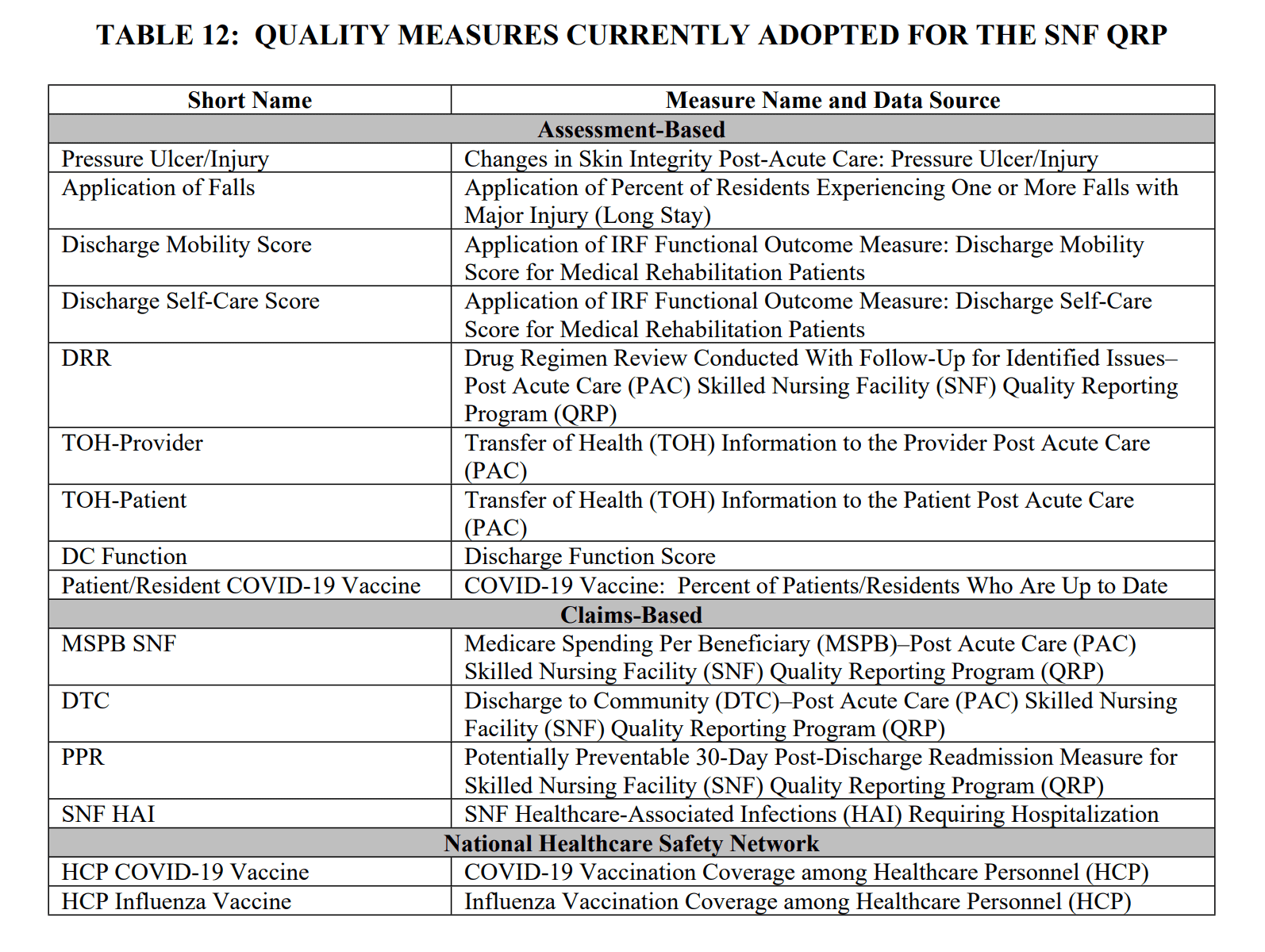
But that does not mean we can sit back and relax. We still have the Measures below in place for 10/1/26 (FY2027).
Other SNF QRP Changes
The Proposed Rule outlines 1 additional changes, 1 minor and 1 major.
- MDS Data Submission and CDC HCSN Deadlines
- MDS Submission on All SNF Residents Regardless of Payor
MDS Data Submission and CDC HCSN Deadlines: (Minor Change)
This Rule proposes to revise SNF QRP Data submission deadlines, as well as submission of info to the Healthcare Safety Network, starting 10/1/28.
- MDS: The current timeframe to correct and submit an MDS for the SNF QRP is 4.5 months after the end of the quarter, creating a lag time of 9 months between when a measure is submitted vs publicly reported. This info is intended for consumer use to make informed decisions about where to receive care, and ends up being outdated.
- CMS wants to decrease the lag time for MDS submission and correction, which will allow for info to be made public sooner
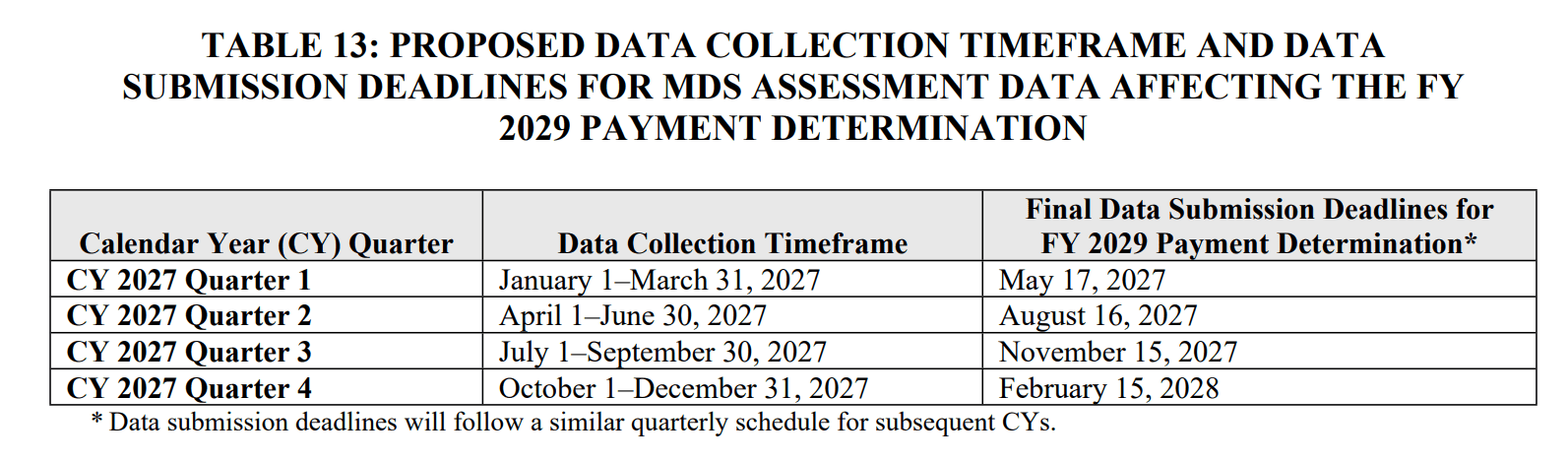
- The Rule proposes starting 10/1/28, MDS submissions and corrections will be due no later than the 15th day of the second month after the end of the quarter, or 45 days after the end of the QRP quarter. (This is not changing rules for MDS completion and submission dates, only the due dates for the QRP program for MDSs that need correction.)
- CMS reported that 97% of all MDS assessments were already being submitted within 45 days, making the new Rule easy to handle for most.
This is what the time-table would look like. Keep in mind that the “old way” and “new way” will collide in May 2027, with due dates for Q4 2026 (old way) and Q1 2027 (new way) assessments.
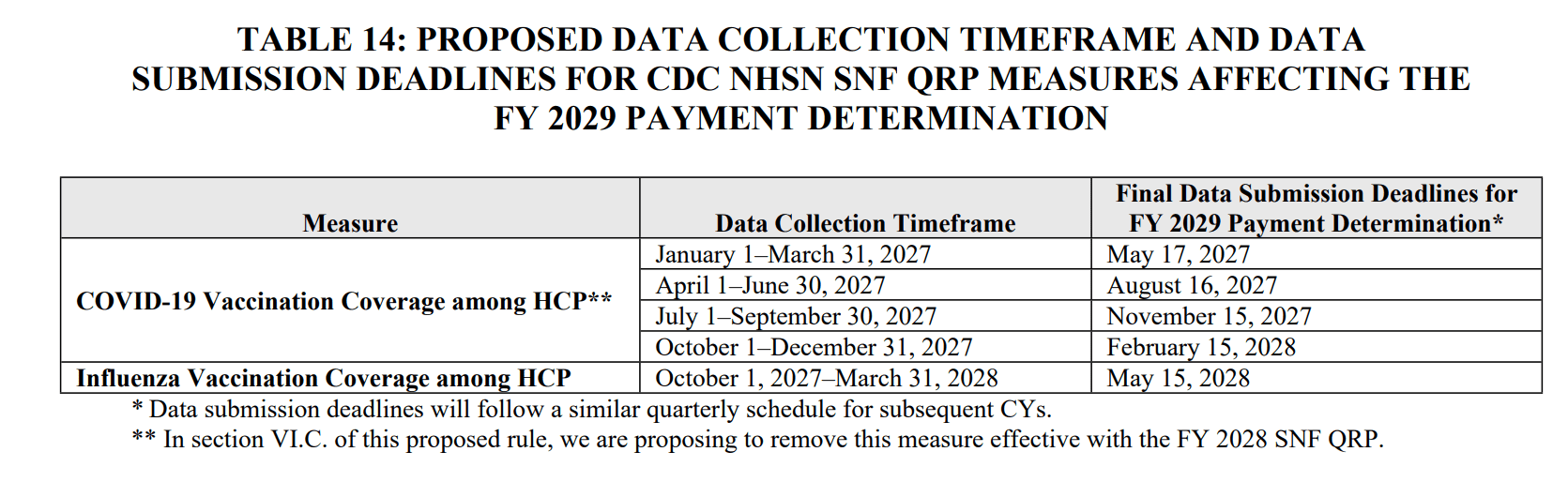
CDC National Healthcare Safety Network Data Submission Deadlines: This Rule proposes to revise the Data submission deadlines similar to the above. This would be the new reporting timeline.
MDS Submission on All SNF Skilled Residents Regardless of Payer: (Major Change!)
The Rule proposes that starting with the FY2031 QRP, non-Part A residents that are receiving skilled care will follow Part A rules for MDS completion and submission.
- Traditional Medicare Part A assessments continue unchanged
- Non-traditional Part A residents receiving skilled care will require a PPS 5-Day and an End of PPS Discharge MDS (ie: Medicare Advantage, Managed Care, Commercial, private plans, etc) for completion AND submission
- Starts with admissions on 10/1/29 or later. Interrupted Stay MDS rules will apply.
- These MDS assessments will count toward SNF QRP compliance rate of 90% of the assessments submitted must be 100% complete, or a 2% payment penalty is imposed. That’s a whole lot more MDS assessments to ensure are 100% complete (no dashes)
- Changes to the MDS can be found in the above MDS Section
- CMS provides the definition of “skilled residents,” modeling Medicare Part A Chapter 8 of the Medicare Benefit Policy Manual:
This will be a major change for many reasons….
Obvious reasons include:
- Increased workload for MDS Nurses with scheduling, completing and submitting each assessment
- The IDT will have additional interviews to complete for both admission and discharge
- The IDT will have “more of Section GG” for documentation, tracking and coding.
- For some SNFs with a healthy skilled population, this could double current MDS tasks.
Some SNFs may currently be completing (not submitting to CMS) a 5-Day PPS assessment for billing purposes only for payors that use a PDPM model and need a HIPPS Code for billing, but the new rule will require a 5-Day AND an End of PPS MDS for all residents, whether payment is via PDPM or “level” contracted rate.
Short-term Rehab residents with insurance that is not PDPM-based may currently only have an Entry and Discharge MDS if the stay is under 14 days, as no other assessments are currently required. Under the new rule, these residents will now need the 5-Day and End of PPS completed and submitted regardless of length of stay,
Some not-so obvious reasons include:
- Therapists know all too well that Managed Plans often “cut” resident therapy services (which ends the skilled coverage) before full gains have been made. These residents are not given the same opportunity that traditional Medicare offers. If CMS is going to use the MDS data to compare non-Medicare length of skilled coverage or progress from admission to discharge, to Medicare Part A residents, “things” may not line up!
- Is therapy being delivered in the same manner to Medicare vs Managed Medicare residents? What is the average treatment time? What is the mode of therapy? Do non-Medicare residents have more group and concurrent therapy? We know the answers, but does CMS?
It will all come out in the data….. Something to look forward to?
On to the last Quality Measure Program….
SNF Value-Based Purchasing Program (SNF VBP)
The SNF VPB Program is a “pay for performance” program (“pay for outcomes”) and works by withholding 2% of all SNFs’ Medicare Part A payments to fund the program, and then allows for an opportunity for SNFs to recoup part of the 2% by demonstrating “success” with the established Measures. CMS redistributes approximately 60% of this back to SNFs as “incentive payments” to encourage improvements in the quality of care provided to Medicare beneficiaries (and yes, CMS keeps the remaining 40%).
Current SNF VBP Measures
Though there are no new measures in this year’s Proposed Rule, we have plenty to work with!
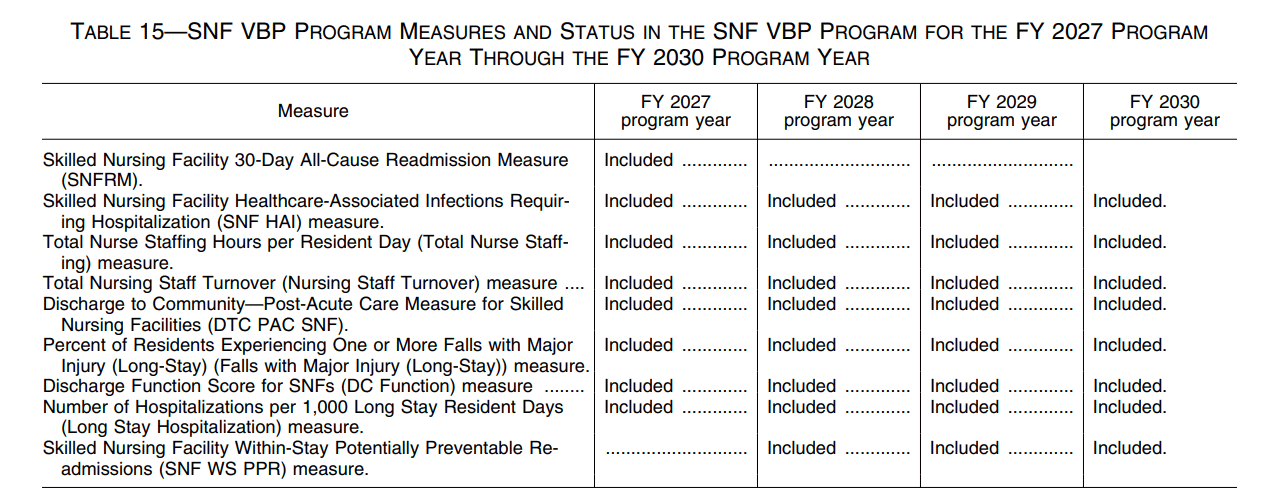
This once tiny little QM program now has 9 Measures to track. The timeline of all the VBP Measures are listed below.
It is important to note that the Program Year is synonymous with “payment impact year,” which follows 2 years after the “Performance Year. Even though some of these dates feel a bit “far off,” we need to pay attention to the Performance Year, as this is the “data collection start date.”
Once the Program Year hits, it’s too late to do anything about the data... and unlike the SNF QRP where “outcomes” do not determine payment, the VBP Measures ARE tied to reimbursement.
- The Measures below have been in data collection mode and all have an impact on payment as of 10/1/26.
- Only 2 of the Measure rely on the MDS 100%: DC Function Score and Falls with Major Injury.
- The remaining measures are claims-based, or use a combination of MDS info with Payroll Based Journal information.
- The last Measure on the list will replace the 1st Measure for payment impact 10/1/27. Both are claims-based and have to do with hospital readmissions.
Since 2 of the above Measures are also in the SNF QRP, CMS proposes to change the snapshot, or data collection dates, for better alignment. The DC Function Score Measure and the Falls with Major Injury measure will move to a shortened snapshot date of 4.5 months to 45 days, as described under the QRP. For FY2027, this will move the snapshot dates from February 15th (4.5 months after 9/30/27) to November 15th (45 days after 9/30/27).
SNF VBP Measure Performance Standards
The Proposed Rule released the Achievement Threshold and Benchmark for each of the VBP Measures as shown below. This information is used to determine the facility incentive multiplier… A.K.A. the variable that will increase or decrease your Medicare payment rate.

summary
October 1st changes signify another year around the SNF sun….
Proposed items we have to look forward to…
- Part A rates are up…… depending on where you live…. check your Wage Index!
- No PDPM changes yet…. waiting for the Case Mix Creep….
- SNF QRP requirement to complete PPS admission and discharge MDS assessments for all residents receiving skilled care, not just Medicare Part A residents. Soon CMS will have lots of data for comparison. Take time to assess your therapy and MDS practice patterns to ensure everything is “in order” when comparing Medicare A to Managed Care residents.
- MDS questions added to accommodate coding to identify PPS assessments for non-Medicare residents.
- 2 SNF QRP (Part A) COVID Measures leaving
- SNF QRP and VBP submission and correction timeframes closing the gap from 4.5 months to 1 month + 15 days so the public has more timely information.
additional resources
HERE is a link to the Proposed Rule PDF Version
HERE is a link to the Federal Register Proposed Rule
HERE is a link to the CMS Fact Sheet
PDPM Calculators and Resources HERE
If you have any questions, send them to our Just Ask Q&A Team and we will get your questions answered.
Thank you for all you are doing to provide the best care to the geriatric population!
In your corner,
Dolores
Dolores Montero, PT, DPT, RAC-CT, RAC-CTA
President | Montero Therapy & MDS Resource Team
MonteroTherapyServices.com