
The “Case-Mix Creep” may be in the Skilled Nursing Facility (SNF) setting. Yikes!
The title sounds like we may need to call 911 to either report a suspicious character lurking about, or to request medical assistance for some new disease variant.
Either way, the term “Case-Mix Creep” is an attention-grabber, and has a specific definition rooted in healthcare reimbursement.
Case-Mix “Without the Creep”
In the SNF setting, we know that the term “Case Mix” represents, for the most part, the acuity of our resident population. This acuity is determined based the Minimum Data Set (MDS) score. Each resident receives a score with a numerical value, or Case Mix Index (CMI) value, for each of the 5 Components in the Patient Driven Payment Model (PDPM). Think of each Component (PT, OT, Speech, Nursing and Non-Therapy Ancillary) as being a ladder, and based on how the MDS questions associated with that ladder are answered, the resident will land on a rung. That rung, or Case Mix Group (CMG) has a Case Mix value. Higher values suggest the resident needs a higher level of care or may need more resources.
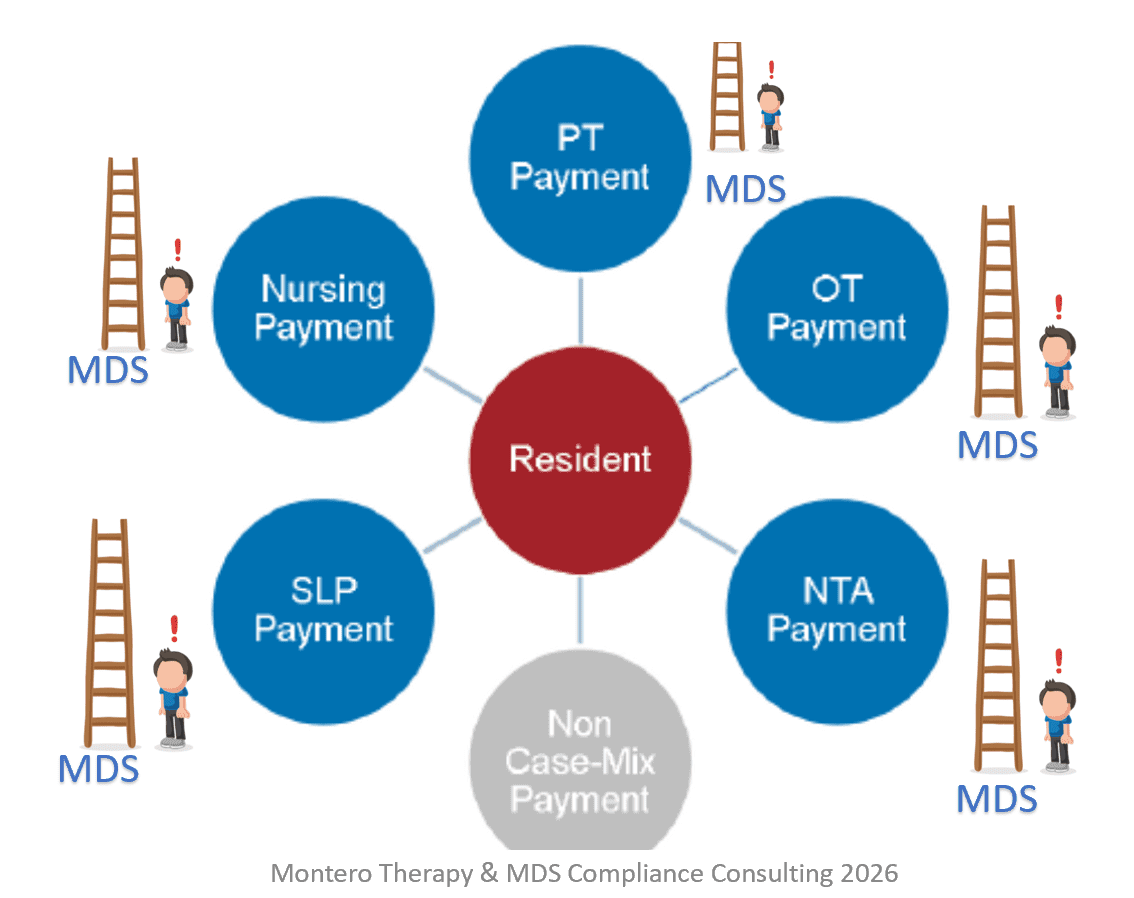
For example, a resident on the Nursing ladder with a Fever and Pneumonia requires more staff time, monitoring and resources than a resident who is on oxygen, and as a result, will have a higher Case Mix Group acuity and numerical value….. higher on the ladder.
When we look at our resident population as a whole, we can determine what the average CMI “score” for each ladder is by placing each resident on “their rung” based on individual scores and then getting an average for the group. We can also look at our resident population in different groups to determine average CMI values. For example, the average CMI can be calculated for different payors, Medicare Part A vs. Managed Medicare vs. Medicaid vs Private Pay.
Knowing the Case-Mix values for your resident population extends beyond reimbursement. For example, knowing the average or acuity for each of your units will help ensure appropriate staffing is assigned, as a unit with higher acuity (higher CMI average) may need more staff.
Case-Mix “With The Creep”
The term Case-Mix Creep was introduced and discussed by the Center for Medicare and Medicaid (CMS) in the FY2027 SNF Prospective Payment System (PPS) Proposed Rule recently released, and has caused a stir, particularly in the way CMS proposed to deal with it.
CMS stated there was an observed “upward creep” in the Case Mix averages for Part A residents, and had Acumen, a CMS contractor, evaluate the data to determine if the “creep” reflected a “real change in resident acuity” or a “nominal change based on MDS coding.”
In other words, Acumen was asked to determine which PDPM ladders residents were climbing up, and why. Was it because residents truly were more acute in certain areas, or was there a change in MDS coding practices, termed “upcoding.”
Acumen looked at data from FY2018 to FY2024.
The 3 creeping PDPM Components identified were Speech, Nursing and NTA, with the associated MDS questions as follows:
- Speech Component: Swallowing Disorder Section K0100 increased from 4% to 21%
- Nursing Component: Depression / Mood Interview Section D (PHQ) from 4% to 19%
- NTA Component: Malnutrition Section I5600 from 5% to 47%
What would these numbers look like if, instead of using FY2018 to FY2024 data, Acumen used FY2024 data forward? HERE is a link to the Acumen Report
How CMS Plans to Handle “the Creep”
Adjustments….
In the Proposed Rule, CMS asked providers for feedback on the methods they presented to deal with the creep. The proposed methods included applying an adjustment to the rates of PDPM Components:
- Individually based on creep
or
- Equally across all components
These adjustments may feel all too familiar. When we transitioned from the RUG payment system to PDPM on 10/1/2019, there was a hiccup in maintaining budget neutrality. The same 3 PDPM Components that are showing creep now, had “Case-Mix Leap” in the 1st year of PDPM, requiring a “recalibration,” or requiring SNFs to “payback” the 5% jump to CMS over a 2 year period. This article helps explain what happened at that time.
Even though Acumen’s report indicates adjusting for the COVID years, those of us in the field know how “Twilight Zone” those years were. Maybe we can hold off on any adjustments for now, reassess FY2024-FY2026, and make decisions based on more solid ground?
a Learning Curve
Maybe “real creep” or “upcoding creep” are not the only 2 options to choose from in the Case-Mix Creep question. It can’t be that black and white…. that either residents are sicker, or MDS items are being coded that are not true.
It’s very likely that other factors played into shifting CMI values. PDPM was brand new to everyone who had been playing by RUG payment system rules for 2 decades, and there were many moving parts to the new system, some of which everyone has not yet caught up with.
Factors contributing to a coding adjustment period include:
- Nursing services were now out from under the shadow of Rehab services. Coding any and all items that contributed to the Nursing Case Mix Group for PDPM was key, where in the RUG system, if a resident was in a Rehab RUG, omitting an item under the Nursing Category would not impact the score, as the Rehab RUG prevailed.
- Malnutrition and Swallow Disorder would both fall in this category.
- Items now tied to NTA points via adding ICD-10 Codes to Section I8000 were likely not seen as a priority prior to PDPM. For example, morbid obesity or BMI ICD-10 codes may have been moved to the bottom of the list and did not make the MDS, even though present
- A rise in the NTA Case-Mix average could be items like this that were always present, though initially not coded, and it took time for the learning curve to kick in.
- Items that were potentially present and overlooked for coding include “Malnutrition” and “Malnutrition Risk.” Those residents likely had assessments, care plans and interventions to manage malnutrition, though it may have been omitted in error, as other items took priority
- Therapy professionals began helping with BIMS and Mood Interviews, as well as Section K coding for Swallow Disorders.
- That’s all 3 of the items mentioned above.
It takes time to learn all the ins and outs of a new process, and some of that “true learning” didn’t happen until after the Public Health Emergency ended.
Maybe some of this “creeping” is true learning.
It’s called a learning curve for a reason!
If you have any questions, send them to our Just Ask Q&A Team and we will get your questions answered.
Thank you for all you are doing to provide the best care to the geriatric population!
In your corner,
Dolores
Dolores Montero, PT, DPT, RAC-CT, RAC-CTA
President | Montero Therapy & MDS Resource Team
MonteroTherapyServices.com